Pigment Dispersion Syndrome
As noted in the section on glaucoma, the vast majority of people with the disease have the open angle type, and most of these have what is known as primary open angle glaucoma, or POAG. The main feature of POAG, aside from elevated intraocular pressure (IOP) and visible damage to the optic nerve, is an otherwise normal eye. In other words, there are no other identifiable abnormalities to explain either the pressure or optic nerve damage. The cause or causes of POAG are largely unknown, though numerous genetic defects are being studied for their role in the disease.
A significant number of patients with open angle glaucoma have special forms of the disease, known as secondary open angle glaucomas. In these conditions, there are identifiable abnormalities responsible for the elevated intraocular pressure and associated damage. One such condition, pigment dispersion syndrome, is described below.
Pigment Dispersion Syndrome and Pigmentary Glaucoma
Pigment Dispersion Syndrome (PDS) with pigmentary glaucoma is another relatively common form of secondary open angle glaucoma. This condition typically occurs in younger patients, between the ages of 20 and 45. Patients are more often male and tend to be nearsighted.
In PDS, small pigmented (brown colored) granules are rubbed off the back of the iris due to abnormal contact between the iris and the zonules, the fibers which hold the lens in place. This is believed to be caused by an abnormality of iris anatomy in which the iris is positioned too far back within the eye. Why this develops is not known. The released pigment then floats about the eye, being deposited in multiple locations, including within the trabecular meshwork and drainage channels where it causes damage and may lead to elevated IOP.
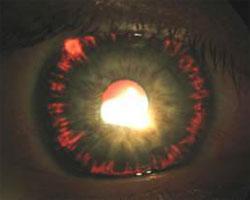
Diagnosis of PDS is made by identifying typical patterns of pigment deposition within the eye, as well as other common features. Pigment is frequently seen on the cornea in a spindle-shaped pattern (known as a Krukenberg’s spindle) and may be seen on the front or back surface of the lens. Often quite dense and dark, pigment is always found within the trabecular meshwork. Slit-like defects in the iris, known as transillumination defects, are typically seen to some degree, and represent areas where pigment has been extensively worn away by rubbing against zonules. The front of the eye, called the anterior chamber, is often abnormally deep in appearance due to the backwards displacement of the iris.
IOP in pigmentary glaucoma can fluctuate widely, often becoming quite high. In fact, IOP “spikes” have been noted to occur spontaneously or, in some cases, after exercise due to sudden release of large amounts of pigment. While most types of glaucoma seldom have any acute symptoms, these rapid elevations of pressure can lead to pain and blurred vision, at times with halos seen around lights. Anyone diagnosed with PDS should report such episodes to their eye doctor, as adjustments in treatment might be indicated.
Not everyone with PDS develops elevated IOP or glaucoma. In fact, there appears to be no direct correlation between the amount of pigment in the trabecular meshwork and the level of intraocular pressure. The reasons for this are not understood, but it is believed that pigmentary glaucoma requires more than just pigment release, that there must be some other abnormality of the drainage channels that has not yet been identified. If PDS is identified during an examination and the optic nerves and IOP are normal, a few additional pressure checks may be performed over the next several months. If IOP remains normal over multiple visits, observation every 6 to 12 months may be indicated.
Treatment of pigmentary glaucoma is similar to that of other types of open angle glaucoma. Medications are usually the first option, often with multiple medications required to control pressure fluctuations. Laser trabeculoplasty can have a very good effect in PDS, often dropping the IOP significantly. The drop in pressure from trabeculoplasty is temporary however, and IOP may begin to elevate again within a few years. Furthermore, patients with PDS occasionally experience substantial spikes in IOP after laser treatment, and at times pressure elevation may be sustained. Therefore, caution must be taken when performing this procedure. Finally, glaucoma filtering surgery such as trabeculectomy can be performed quite successfully.
Free Lasik Screening
Call 520-355-7501 or Enter Your Information Below!
Please do not submit any Protected Health Information (PHI).
More Categories