


What Are the Risk Factors of Glaucoma?
A number of risk factors for the development of glaucoma have been identified:
-
High intraocular pressure: IOP above 21 is considered high, and with increasing pressure comes an increased risk of glaucoma. However, not all high pressure will lead to glaucoma.
-
Race: African Americans are five to six times more likely than Caucasians to be affected by the disease, which tends to be more severe and progress more quickly in this population. Latinos are also at greater risk than Caucasians. The reasons for these racial differences are not well understood but are most likely genetic.
-
Family History: History of glaucoma, particularly in a first-degree relative, i.e. parent or sibling, increases one’s risk. The genetics of glaucoma, however, are usually not simple, and there is no way to predict which family members will be affected.
-
Age: Glaucoma is uncommon under 40, but risk increases with each decade of life.
-
Blood Pressure: High blood pressure has been associated with increased intraocular pressure in some studies, but it remains unclear exactly how significant this association is clinically.
Low blood pressure may be a risk factor for glaucoma progression, particularly in patients with low tension glaucoma, a form of open-angle glaucoma in which the pressure is in the normal range, often quite low.
-
Sleep-associated breathing disorders: Disorders such as sleep apnea, may be a risk factor, particularly for low tension glaucoma, again due to abnormal blood flow to the optic nerves.
Other possible risk factors include diabetes and myopia (nearsightedness), however studies have provided inconsistent results as to the degree of association with these factors.

Why Our Facility Is a Great Glaucoma Management Center for You
We know that you have a choice of teams and locations for your care. Our team of experts look forward to providing the highest quality care. Our experienced team, high-tech equipment, and personalized care provide you with the best outcomes for your vision.
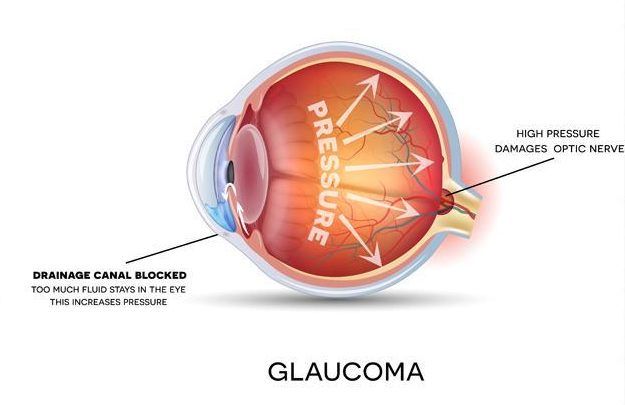
Scientist are not entirely sure what exactly causes Glaucoma. Ultimately the passages that allow the fluid within your eye to drain are blocked. Because of that, fluid builds up in your eye and causes an increase in pressure on the optic nerve. The optic nerve and blood vessels are damaged by the increased pressure, which can result in vision loss.
Glaucoma can cause blindness, but it can be prevented. If it is diagnosed at an early stage, the damage can be controlled. If treatment is delayed, you are likely to lose peripheral vision first and then the central vision, which may result in complete blindness.
Glaucoma often does not have obvious symptoms. Additionally, symptoms may not show until it is already too late.
If you have open-angle Glaucoma, the initial symptom might be vision loss – which is a sign of damaged optic nerve.
If you have closed-angle closure Glaucoma, initial symptom may be blurry vision. You might also see rings or halos around lights. You may experience pain or strain in your eye and they may also get red.
Glaucoma is usually broken down into two major categories: open-angle glaucoma and closed-angle glaucoma.
In open-angle glaucoma, the drainage canals are correctly formed but are slow clogging, resulting in increased eye pressure.
In closed-angle glaucoma, the entrance to the trabecular meshwork becomes blocked by the iris, which assumes an abnormally forward position. This causes the drainage canal to become narrow and eventually close. Unlike symptom-free open-angle glaucoma, this condition, sometimes called “narrow-angle glaucoma,” often presents suddenly, with pain, red eye, tearing, and colored haloes around lights. Vision can be lost quickly, and urgent treatment is required.

