It must be remembered that the optic nerve damage and subsequent loss of vision caused by glaucoma cannot be reversed. Thus, the point of surgery is not to improve vision, but rather to prevent further vision loss. Currently there is no glaucoma treatment that can restore vision already lost to the disease. For this reason, early diagnosis and treatment are vital. We recommend reading the section about glaucoma before continuing here.
This section describes trabeculectomy, the most commonly performed surgical procedure used to treat most forms of glaucoma.
Introduction
Also known as a “trab,” “filter,” or “bleb surgery,” this is the most commonly performed glaucoma surgery in the United States. In this procedure, a small canal is surgically created through the sclera, or white of the eye, in order to drain the aqueous humor, the intraocular fluid which fills the front of the eye and which generates the intraocular pressure. For simplicity, think of glaucoma as being caused by a clogged drain. Aqueous humor is constantly being created but cannot escape quickly enough, building up pressure and damaging the optic nerve. The trabeculectomy canal gives the fluid a low resistance means of escape, leading to lower, better controlled pressure. The fluid which leaves the eye drains into a space beneath the conjunctiva, the clear membrane which covers the white of the eye, before being reabsorbed into your bloodstream. This fluid is different from tears and the eye’s natural external moisture and will not drip onto the face.
Procedure in Detail
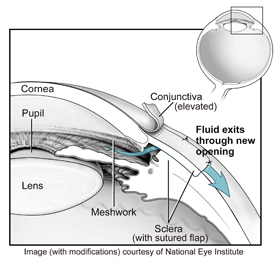
Trabeculectomy is generally performed as an outpatient procedure under local anesthesia with IV sedation- you will be awake but relaxed and will experience no discomfort. After the skin around the eye is cleansed, a surgical drape is placed over the eye to maintain sterility. A small device known as a lid speculum is placed in order to hold open the eyelids during the procedure. The eye is turned downward, exposing the conjunctiva and sclera above the cornea, which is where the surgical site will be located. A small incision is made in the conjunctiva, which is then carefully lifted and separated from the sclera.
A half-thickness flap of sclera is then dissected up to the edge of the cornea. The flap will later be sutured back into place, where it will function as a valve controlling the flow of fluid from the eye. Near the base of the flap a small metal stent, known as an EX-PRESS® glaucoma shunt, is inserted through the sclera and into the anterior chamber of the eye. This tiny tube creates the actual opening into the eye through which the aqueous humor is able to escape. Some surgeons prefer to simply punch a small hole in the sclera instead of placing this shunt. However, the standardized 50 micron opening of the shunt provides a more controlled means of draining aqueous humor from the eye. Studies have shown that the shunt promotes faster visual recovery and reduces the rate of some early post-operative complications. There are certain situations, however, where the EX-PRESS® shunt cannot be safely placed or is otherwise contraindicated. In such cases we revert to the punch technique. The EX-PRESS® shunt is fully MRI safe, having been tested in magnetic fields up to 3 Tesla.
Once the surgeon determines that the opening is adequate, the scleral flap is sutured back into its original place. The sutures are tightened just enough to allow the right amount of aqueous humor to leak out of the eye. If the sutures are too tight then flow will be inadequate and the IOP will remain too high. Sutures tied too loosely can result in a very low pressure, which is also undesirable. Obtaining just the right amount of flow is sometimes challenging during surgery, but fortunately adjustments can be made in the days and weeks following the procedure, as described in the next section. Once the surgeon is happy with the flow of aqueous, the initial conjunctival incision is meticulously sutured to create a watertight seal. The end result is a small blister of fluid, known as a “bleb,” which collects around the surgical site, hidden from view by the upper eyelid. This fluid ultimately drains back into the bloodstream.
Once surgery is completed, the eye is generally tightly patched and protected by a hard, plastic shield overnight. There is usually minor discomfort and itching. Significant pain is uncommon.
The Day after Surgery
The following morning you will come to the office for a post-operative check up. The patch and shield will be removed, and the surgeon will check your vision, IOP, and the appearance of the eye, including the bleb. The shape and size of the bleb can tell your physician how well fluid is flowing from the eye. At this point, instructions regarding acceptable levels of activity and use of postoperative eye drops, including steroids and antibiotics, will be given. It is very important that the drops be taken as prescribed in order that the surgery heals properly. The degree of allowable physical activity, including the ability to drive in the days following surgery, depends on each patient’s unique situation and must be judged individually. In general, strenuous activity, heavy lifting, and bending over should be avoided for the first one to two weeks.
The First Few Weeks after Surgery
Discomfort is generally mild in the first weeks after surgery. The eye may feel a bit sore, and typically there is a scratchy, foreign body sensation due to stitches. Vision is quite variable in these early days, ranging from almost normal to quite blurred. Don’t be alarmed if vision is poor initially, as acuity generally returns to preoperative levels after a few weeks, though may take longer and typically fluctuates quite a bit initially.
You will be monitored closely during the first two to four weeks following surgery, as this period of time is the most critical to achieving a successful outcome. Immediately following surgery, the eye will begin to heal. Our bodies were designed to heal themselves, to repair a wound by growth of new tissue and development of a scar. Yet we have purposely created an opening into the eye which we do not want to heal. If the opening scars closed, the surgery fails and we will be back where we began, with high pressure. Risk factors associated with increased scarring include young age, dark pigmentation (African Americans, Latinos), ocular inflammations such as uveitis, and prior surgery involving the conjunctiva, such as previous glaucoma or retinal surgery.
A number of measures are taken to slow down and limit the healing process. First, medications such as mitomycin-C (MMC) or 5-fluorouracil (5-FU) are nearly always used during surgery. These medications, known as antifibrotics, slow the growth of scar tissue on the surface of the eye. Following surgery, additional antifibrotic drugs are given in the form of eye drops to limit scarring and keep the fluid flowing. The primary medication used is a corticosteroid and is commonly prescribed to be taken four times per day, though occasionally more frequent use is required. Corticosteroid drops are often continued in a tapering dose regimen for 8 to 10 weeks following surgery. Antibiotic drops will also be prescribed during the first 1 – 2 weeks. Occasionally, other medications may also be required.
If healing is found to occur too quickly, additional antifibrotic therapy may be provided in the form of 5-FU injections beneath the conjunctiva. The surface of the eye is numbed with drops and the medication is injected just under the conjunctiva near the bleb. If necessary, the tip of the needle can be used to very gently break up scar tissue under the conjunctiva. This procedure is well tolerated by most, with only minor discomfort or burning.
If the flow of aqueous fluid is too slow, and pressure therefore too high, the sutures placed on the scleral flap can be loosened or removed in order to allow more fluid to flow out of the eye. The means of adjusting these sutures depends upon how they were placed at the time of surgery. Some sutures are “releasable,” meaning that they can be easily grasped with forceps in the examination room of the office and easily removed from the eye. Again, this is done with eye drop anesthesia and causes no discomfort. Other sutures are “fixed” and must be cut in place using a laser in the doctor’s office. Regardless of how the sutures are placed, the result of removing or cutting them is usually an increase in aqueous flow out of the eye and a significant drop in the intraocular pressure.
On the other hand, it is not unusual for the IOP to run rather low during the first few post-operative weeks. This is seldom a significant problem, as pressure typically rises as the eye heals, settling at an appropriate level. In rare cases, if the IOP does not rise appropriately, a return to the operating room may be necessary to place additional sutures in the scleral flap.
Trabeculectomy may lead to a change in the eye’s refractive state, requiring a change in eyeglasses prescription. The eye is usually well healed and stable enough for this at about 8-10 weeks after surgery.
Months to Years after Surgery
Trabeculectomy is generally a very effective procedure for IOP reduction, with an 85 to 90% chance of maintaining intraocular pressure at the desired level after one year. In approximately half of these successful cases no further use of glaucoma medications is necessary. The other half must continue at least one medication to maintain the desired level of IOP. As the years pass it is not unusual for IOP to begin to increase, possibly necessitating the use of medications, or additional surgery. In approximately 10% to 15% of cases, surgery fails to adequately control the IOP beyond the early postoperative period. Additional surgery may then be performed to reach the desired level of pressure within the eye. Another trabeculectomy may be an option, or a tube shunt procedure may be preferred (see article on Glaucoma Drainage Devices).
Patients who have undergone trabeculectomy have an increased lifetime risk of developing an infection inside the eye. Known as endophthalmitis, this kind of infection can seriously harm the eye and lead to loss of vision. The increased risk is due to the opening made in the eye; just as fluid can more easily escape the eye, bacteria can more easily enter. While this risk is generally low, anyone who has undergone trabeculectomy is advised to contact their ophthalmologist immediately if the operated eye ever becomes significantly red or painful, or if vision suddenly decreases. For this reason, the use of contact lenses after trabeculectomy is discouraged.
Risks of Surgery
All surgical procedures carry some risk of complications. Some risks are common to all procedures and patients, and others are more specific to certain types of surgeries or to patients with particular conditions. A thorough explanation of complications will be provided with a surgical consent, should you choose to have surgery, and your physician will review the specific issues you may face based upon your unique circumstances.
Complications
Complications of trabeculectomy can be divided into early (days to weeks after surgery) or late (months to years after surgery) problems:
Early complications:
- Failure to control IOP, as described in detail above
- Bleeding within the eye (hyphema), usually resolves within one week
- Low intraocular pressure (hypotony) resulting in retinal damage (maculopathy), fluid or blood accumulation within the layers of the eye (suprachoroidal fluid or hemorrhage), or shallow anterior chamber
- Wound leak, may require additional sutures
- Infection within the eye (endophthalmitis)
- Loss of central vision, rarely severe loss
Late complications:
- Cataract (clouding of the lens of the eye)- development or progression of cataract is fairly common after trabeculectomy, and may necessitate surgery for cataract removal in subsequent years.
- Drooping eyelid (ptosis)
- Bleb leak, due to breakdown of conjunctiva over the bleb, can cause hypotony (see above)
- Infection within the eye (endophthalmitis), risk increases with bleb leak
Alternatives to Trabeculectomy
As with most diseases, there are a number of treatment options for glaucoma. As previously noted, surgery is usually considered when medications and laser trabeculoplasty have failed to adequately control IOP. Trabeculectomy, while the most common surgical procedure for glaucoma, is not the only option available. Other surgical procedures may be considered based upon the type of glaucoma, condition of the eye, and level of IOP required. Your surgeon will discuss alternatives for your particular situation, as appropriate. Some of these procedures are detailed in other articles.
One procedure of note is known as a XEN gel stent. The XEN is a tiny tube, about the size of a human eyelash, that can be implanted through the sclera to allow aqueous to drain from the eye, forming a filtering bleb similar to that with a trabeculectomy. However, because there is far less tissue manipulation and no sutures, healing and visual recovery are faster, and discomfort is less. Furthermore, the overall risk of certain complications, including overly low IOP, is reduced. On average, the XEN does not lead to IOP as low as that which can be achieved by trabeculectomy. But for patients who do not require an extremely low pressure, XEN may be a good and safe alternative. Your surgeon will discuss the XEN if he/she believes you are a good candidate for this procedure. More information about the XEN can be found online at xengelstent.com.